
The emergence of Covid-19 has led to an unprecedented response from governments around the world, including in Saudi Arabia. This is the first time that social interventions have been deployed on a global scale with the view to fundamentally change the primary infection curve and slow infection growth. This fundamental change has significant impact on the health sector, more used to dealing with uncontrolled demand (Figure 1) with relatively rapid growth and recovery phases. Social interventions will significantly reshape the infection curve (Figure 2), extending response and require policymakers to consider a range of different actions. In the coming series of blogs, we will consider some of the potential tactical response models, reflecting the impact of the social interventions taken across Saudi Arabia. That will include a review of current approaches and solutions that should be considered to mitigate the risk during the outbreak and once normal services resume.
While the current focus has rightfully been on dealing with emergency cases, other medical services have ceased, at the cost of patient experience, quality of life, and possibly mortality. As this will not resolve quickly, when and how should we start providing a broader range of services? Where should the focus be? In the first of these series on tactical response models, we discuss the foundation of the thinking and while using the term ‘business as usual’ (BAU), we recognize that the impact of Covid-19 will reshape our definition of ‘usual’.
The challenge facing any health system is to meet the needs of the population. During epidemics and pandemics, the focus is always on dealing with managing the immediate impact when large numbers of infected patients requiring care. Flattening of the curve through social interventions has significantly extended the duration of the ‘growth’ phase, with increasing numbers of patients waiting for diagnosis and management. This is particularly concerning for suspected cancer patients or complex patients waiting for urgent elective treatment, especially those requiring access to an Intensive Care bed post-operatively.
Graham Jelley

Director - Healthcare
KPMG in Saudi Arabia
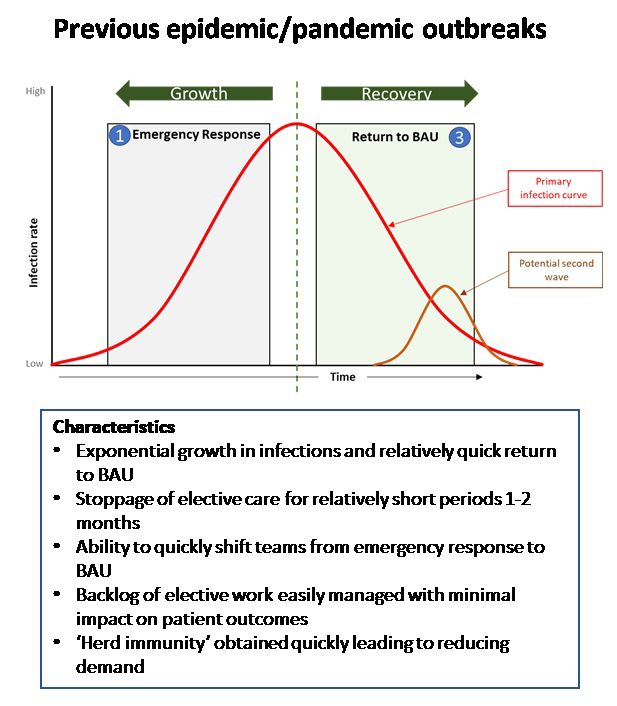
Figure - 1 : Normal curve as monitored during similar outbreaks with an exponential growth phase followed by an equally short recovery phase.
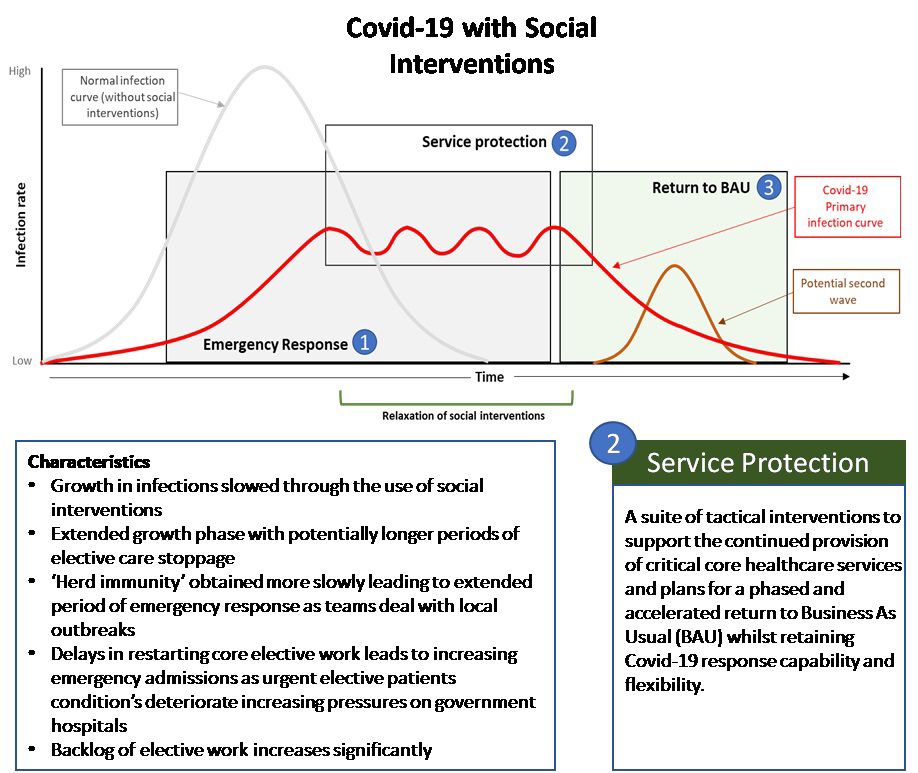
Figure -2 : The expected impact of social interventions.
Health planners and policymakers will need to think differently about their response to Covid-19 with a more active ‘service protection’ phase that bridges the response and return to BAU phase to dynamically maintain a level of core service provision. This is particularly important as Saudi Arabia has just reached the point of partial relaxation of restrictions; this will naturally lead to local spread and outbreaks that need to be actively managed, fundamentally changing the infection curve (Figure 2).
The extended duration of the response requires all health systems to retain agility, to respond effectively to local outbreaks as they occur. that the management actions taken will need to ensure enough capacity to reduce mortality from Covid-19 whilst providing a level of core services that reduce the mortality due to delayed treatment of other patients
This ‘service protection’ phase is an addition to the standard model and covers a suite of interventions that support the maintenance of core healthcare services whilst ensuring sufficient flexibility and capacity to manage the natural demand variances exhibited during any outbreak.
Previous approaches with two relatively short distinct phases are potentially less relevant with the advent of Covid-19 as a further suite of management actions are required to protect some core service provision. Over the next series of blogs, KPMG will consider this ‘service protection’ phase and the portfolio of interventions required to enhance current management approaches and reduce mortality whilst also supporting the transition back to normal services, and the medium-term sustainability of care provision.
